H.6.1 Define partial pressure
Partial pressure is the pressure exerted by a single type of gas when it is found within a mixture of gases
The partial pressure of a given gas will depend on:
- The concentration of the gas in the mixture (e.g. O2 levels may differ in certain environments)
- The total pressure of the mixture (air pressure decreases at higher altitudes)
H.6.2 Explain the oxygen dissociation curves of adult haemoglobin, fetal haemoglobin and myoglobin
Haemoglobin is composed of four polypeptide chains, each with an iron-containing heme group capable of reversibly binding oxygen
- As each oxygen molecule binds, it alters the conformation of haemoglobin, making it easier for others to be loaded (cooperative binding)
- Conversely, as each oxygen molecule is released, the change in haemoglobin makes it easier for other molecules to be unloaded
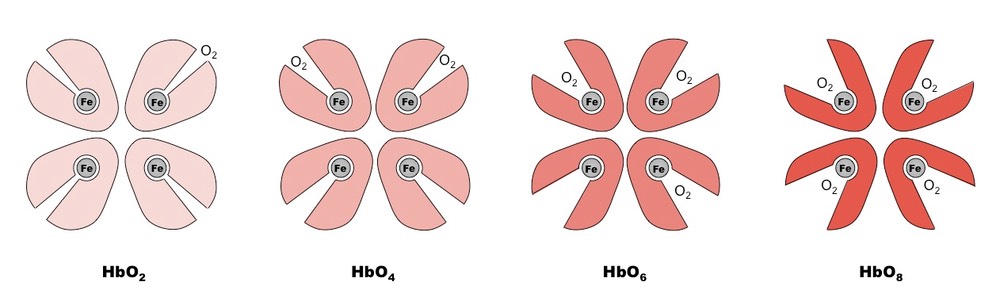
Oxygen dissociation curves show the relationship between the partial pressure of oxygen and the percentage saturation of oxygen carrying molecules
- At low O2 levels (i.e. hypoxic tissues) percentage saturation will be low, while at high O2 levels (e.g. in alveoli) molecules will be fully saturated
- Because binding potential increases with each additional oxygen molecule, haemoglobin displays a sigmoidal (S-shaped) dissociation curve
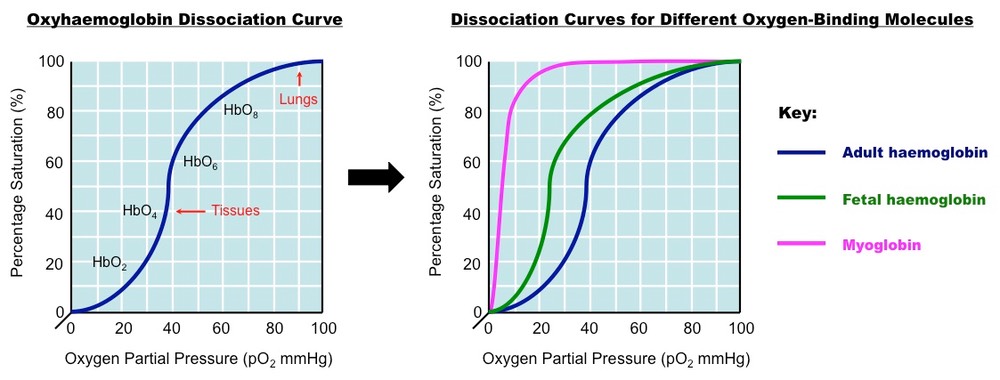
Adult Haemoglobin
- Dissociation curves displays a typical sigmoidal shape (due to cooperative binding)
- There is low saturation of oxygen when partial pressure is low (corresponds to environment of the tissue, when oxygen is released)
- There is high saturation of oxygen when partial pressure is high (corresponds to environment of the alveoli, when oxygen is taken up)
Fetal Haemoglobin
- The haemoglobin of the fetus has a slightly different molecular composition to adult haemoglobin
- Dissociation curve is to the left of the adult haemoglobin curve (indicating a higher affinity for oxygen)
- This is important as it means that oxygen will move from adult haemoglobin to fetal haemoglobin in the capillaries of the uterus
Myoglobin
- Myoglobin is an oxygen-binding molecule found in muscles that is made of a single polypeptide with only one heme group
- Dissociation curve is to the left of the haemoglobin curve and does not display a sigmoidal shape (myoglobin cannot undergo cooperative binding)
- Myoglobin's affinity for oxygen is greater than haemoglobin and becomes saturated at low oxygen concentrations
- Under normal conditions (at rest) myoglobin is saturated with oxygen and will store it until O2 levels in the body drop with intense exercise
- This allows it to provide oxygen when levels are very low (e.g. in a respiring muscle) and so delays anaerobic respiration and lactic acid formation
H.6.3 Describe how carbon dioxide is carried by the blood, including the action of carbonic anhydrase, the chloride shift and buffering by plasma proteins
Carbon dioxide is transported from the tissues to the lungs in one of three ways:
- Some is bound to haemoglobin to form HbCO2
- A very small fraction gets dissolved in the blood plasma (CO2 dissolves poorly in water)
- The majority (~85%) diffuses into the erythrocyte and is converted into carbonic acid
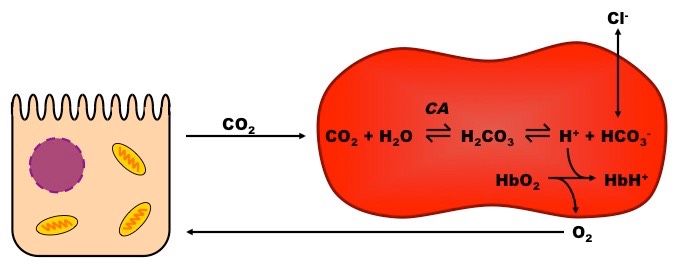
Transport as Carbonic Acid
- When CO2 enters an erythrocyte, it combines with water in a reaction catalysed by carbonic anhydrase to form carbonic acid (H2CO3)
- The carbonic acid then dissociates into hydrogen ions (H+) and bicarbonate (HCO3–)
- Bicarbonate is pumped out of the cell and exchanged with chloride ions to ensure the erythrocyte remains uncharged – this is called the chloride shift
- The bicarbonate combines with sodium ions in the blood plasma to form sodium bicarbonate (NaHCO3), which travels to the lungs
- The hydrogen ions in the erythrocyte make the environment less alkaline, causing the haemoglobin to release its oxygen to be used by cells
- The haemoglobin absorbs the H+ ions and acts as a buffer to restore pH, the H+ ions will be released in the lungs to reform CO2 for expiration
H.6.4 Explain the role of the Bohr shift in the supply of oxygen to respiring tissues
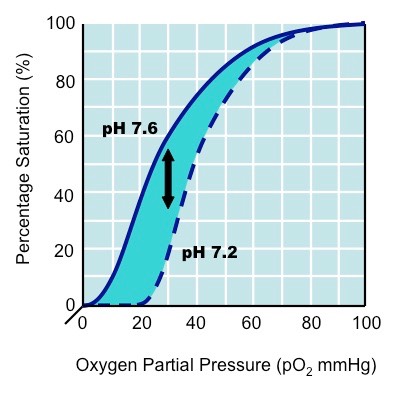
- The oxyhaemoglobin dissociation curve describes the saturation of haemoglobin by oxygen in cells under normal metabolism
- Cells with increased metabolism (e.g. hypoxic tissue) release greater amounts of carbon dioxide into the blood
- Carbon dioxide lowers the pH of the blood (via its conversion into carbonic acid) which causes haemoglobin to release its oxygen
- This is known as the Bohr effect – a decrease in pH shifts the oxygen dissociation curve to the right in tissues
- Hence more oxygen is released at the same partial pressure of oxygen, ensuring respiring tissues have enough oxygen when their need is greatest
The Bohr Effect
H.6.5 Explain how and why ventilation rate varies with exercise
- During exercise metabolism is increased, oxygen is becoming limited and there is a build up of both carbon dioxide and lactic acid in the blood
- This lowers the blood pH, which is detected by chemoreceptors in the carotid artery and the aorta
- These chemoreceptors send impulses to the breathing centre in the brain stem to increase the rate of respiration
- Impulses are sent to the diaphragm and intercostal muscles to change the rate of muscular contraction, hence changing the rate of breathing
- This process is under involuntary control (reflex response) – as breathing rate increases, CO2 levels in the blood will drop, restoring blood pH
- Long term effects of continual exercise include an improved vital capacity
H.6.6 Outline the possible causes of asthma and its effects on the gas exchange system
Asthma is a common, chronic inflammation of the airways to the lungs (i.e. bronchi / bronchioles)
- Inflammation leads to swelling and mucus production, resulting in reduced airflow and bronchospasms
- During an acute asthma attack, constriction of the bronchi smooth muscle may cause significant airflow obstruction, which may be life threatening
- Common asthma symptoms include shortness of breath, chest tightness, wheezing and coughing
Asthma may be caused by a number of variable and recurring environmental triggers, including:
- Allergens (e.g. pollen, moulds)
- Smoke and scented products (e.g. cigarettes, perfumes)
- Stress and anxiety
- Food preservatives and certain medications
- Arthropods (e.g. dust mites)
- Cold air
- Exercise (increased respiratory rate)
H.6.7 Explain the problem of gas exchange at high altitudes and the way the body acclimatises
At high altitudes, air pressure is lower and hence there is a lower partial pressure of oxygen (less O2 in the air)
- This makes it more difficult for haemoglobin to take up and transport oxygen from the alveoli (lower Hb % saturation), meaning tissues receive less O2
- A person unaccustomed to these conditions will display symptoms of low oxygen intake – fatigue, breathlessness, rapid pulse, nausea and headaches
Over time, the body will begin to acclimatise to the lower oxygen levels at high altitudes:
- Red blood cell production increases to increase oxygen transport
- Red blood cells will have a higher haemoglobin content with an increased affinity for oxygen
- Ventilation rate increases to increase gas exchange (including a larger vital capacity)
- Muscles produce more myoglobin and have increased vascularisation (denser capillary networks) to encourage oxygen to diffuse into muscles
- Kidneys will begin to secrete alkaline urine (improved buffering of blood pH) and there is increased lactate clearance within the body
- People living permanently at high altitudes will have a greater lung surface area and larger chest sizes