Cardiac Cycle
Cardiac Cycle
The cardiac cycle describes the series of events that take place in the heart over the duration of a single heart beat
-
It is comprised of a period of contraction (systole) and relaxation (diastole)
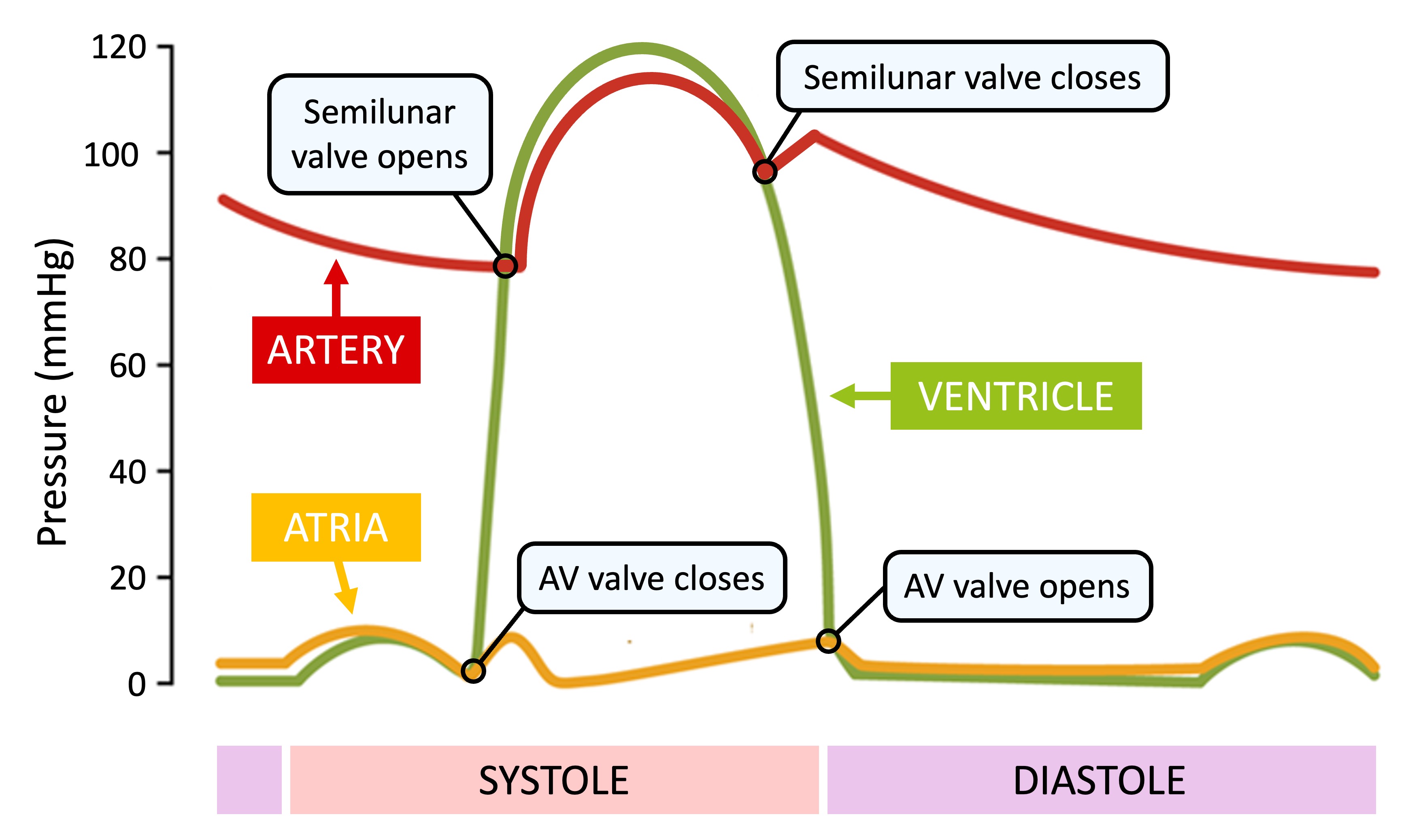
Systole
-
Blood returning to the heart will flow into the atria and ventricles as the pressure in them is lower (due to the low volume of blood)
-
When ventricles are ~70% full, atria will contract (atrial systole), increasing pressure in the atria and forcing blood into ventricles
-
As ventricles contract, ventricular pressure exceeds atrial pressure and AV valves close to prevent back flow (first heart sound)
-
While both sets of heart valves are closed, the pressure rapidly builds in the contracting ventricles (isovolumetric contraction)
-
When ventricular pressure exceeds blood pressure in the arteries, the semilunar valves opens and blood is released into the arteries
Diastole
-
As blood exits the ventricles and travels down the arteries, the ventricular pressure starts to fall
-
When ventricular pressure drops below arterial pressure, the semilunar valves close to prevent back flow (second heart sound)
-
As ventricles contract, ventricular pressure exceeds atrial pressure and AV valves close to prevent back flow (first heart sound)
-
When the ventricular pressure drops below the atrial pressure, the AV valve opens and blood can flow from atria to ventricle
-
Throughout the cycle, the arterial pressure remains quite high as muscle and elastic fibres in the artery wall maintain blood pressure
Cardiac Contraction
Initiation of Heart Beat
The contraction of the heart is myogenic – meaning that the signal for cardiac compression arises within the heart tissue itself
-
In other words, the signal for a heart beat is initiated by the heart muscle cells (cardiomyocytes) rather than from brain signals
The electrical conduction of a heart beat occurs according to the following events:
-
Within the wall of the right atrium is a plexus of cardiomyocytes called the sinoatrial node (SA node) which direct the contraction of heart muscle tissue
-
The sinoatrial node sends out an electrical impulse that stimulates the atria to contract and stimulates another node at the junction between the atrium and ventricle
-
This second node – the atrioventricular node (AV node) – sends signals down the septum via a nerve bundle called the bundle of His
-
The bundle of His innervates nerve fibres (Purkinje fibres) in the ventricular wall, causing ventricular contraction
There are several adaptive advantages to this system of myogenic stimulation:
-
Because cardiac muscle cells are not fused together, they are capable of independent contraction – the SA node acts as a pacemaker to coordinate contractions
-
If the SA node fails, the AV node may maintain ventricular contractions at a lower heart rate
-
This conduction of the signal via the bundle of His ensures there is a delay between atrial and ventricular contractions, allowing time for ventricles to fill with blood
Myogenic Stimulation
Blood Pressure Changes
The contraction of the heart causes changes in blood pressure which results in the flow of blood around the body
-
Pressure in the atria is typically low – this ensures that blood from the veins will fill the heart
-
Pressure within the ventricles fluctuates greatly – it is low during systole and greatly increases during diastole
-
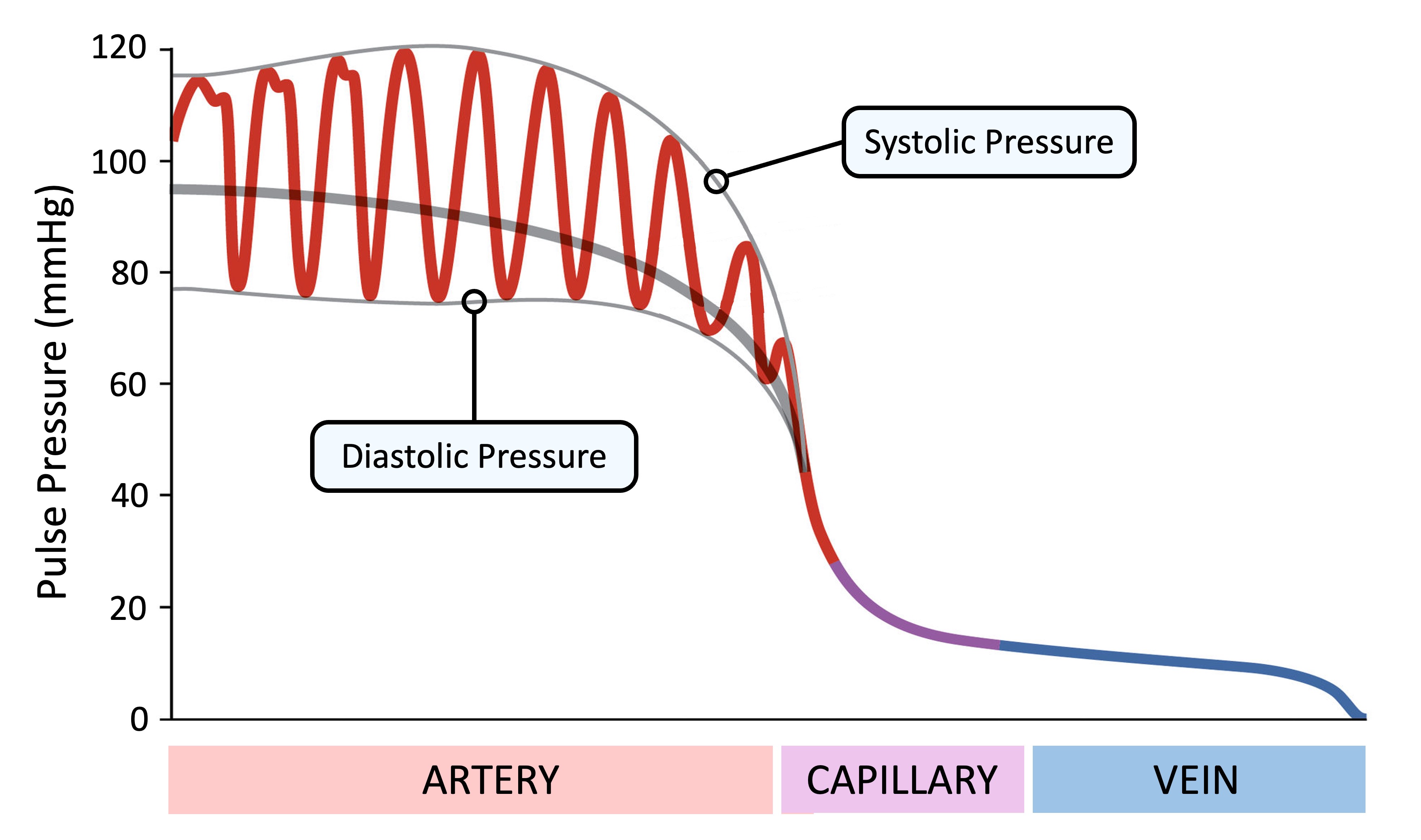
Pressure within the arteries is very high (due to a narrow lumen) but the elasticity of the vessel wall limits the variation experienced with each pulse
-
Typical arterial blood pressure is 120/80 mmHg (120 mmHg = systolic; 80 mmHg = diastolic)
-
As the blood moves further away from the heart the overall pressure decreases, along with the difference between systolic and diastolic pressures
-
There is a neglible fluctuation in blood pressure with each heart beat in the capillaries and veins
Blood Pressure Charts